E-ISSN - 2675-0244
P-ISSN - 1806-3365
RESUMO
Objetivo: desenvolver um aplicativo móvel assistencial e educativo para triagem e gestão do Transtorno do Espectro Autista na Atenção Primária. Métodos: estudo metodológico utilizando o modelo Analysis, Design, Development, Implementation e Evaluation. Dividiu-se nas fases: levantamento de informações (revisão de escopo e de literatura); design e sequenciamento dos conteúdos; adaptação de recursos didáticos. O software Elo foi criado para os sistemas Android e IOS em plataformas de design gráfico, considerando os usuários (profissionais de saúde) e o público (lactentes). Para desenvolvimento do protótipo, seguiu-se as etapas: planejamento, análise de requisitos, codificação e desenvolvimento. Resultados:Foram produzidas 45 telas de acesso do software ELO: login, menu, diagnóstico e link da caderneta da criança, tela de M-CHART-R-definição. Conclusão: O desenvolvimento do aplicativo móvel ELO apresenta-se como importante ferramenta educacional e assistencial para acompanhamento do crescimento e desenvolvimento infantil, identificação precoce e gestão do Transtorno do Espectro Autista na Atenção Primária à Saúde.
DESCRITORES: Atenção Primária em Saúde; Tecnologia em Saúde. Diagnóstico Precoce, Transtorno do Espectro Autista.
Objective: to develop a healthcare and educational mobile application for screening and management of Autism Spectrum Disorder in Primary Care. Methods: methodological study using the Analysis, Design, Development, Implementation and Evaluation model. It was divided into phases: information gathering (scope and literature review); content design and sequencing; adaptation of didactic resources. The Elo software was created for Android and IOS systems on graphic design platforms, considering users (health professionals) and the public (infants). For the development of the prototype, the steps were followed: planning, requirements analysis, coding and development. Results: 45 ELO software access screens were produced: login, menu, diagnosis and link to the child's booklet, M-CHART-R-definition screen. Conclusion: The development of the ELO mobile application is an important educational and assistance tool for monitoring child growth and development, early identification and management of Autism Spectrum Disorder in Primary Health Care.
DESCRIPTORS: Primary Health Care; Health Technology. Early Diagnosis, Autism Spectrum Disorder.
INTRODUCTION
Actions carried out in Primary Health Care (PHC), specifically those aimed at children under 2 years of age, have the potential to prevent health problems in adulthood. An important practice that mitigates risks and identifies delays and vulnerabilities is childcare. Its realization is important as a practice of vigilance, attention, qualified listening, bonding and trust creation. (1) This follow-up care provides from the qualified discharge of the newborn (NB) from the maternity, guidance on the Child Booklet (CB) and the first contact with the PHC, recording information about prenatal care, delivery and childcare consultations , being a means of communication between the family and health professionals. (2)
In the current context, the monitoring of growth and development (GD) has shown weaknesses both with regard to the adequate completion of data in the CH (2-4) as well as in the ideal management of growth and development surveillance, since many consultations are merely restricted to the monitoring of anthropometric values. (5)
In this sense, in the disruption of growth and development monitoring, disorders that interfere with neurodevelopment can bring vulnerabilities to child health that intensify even more if added to the lack of skill and technical knowledge when handling these situations.
Autistic Spectrum Disorder (ASD) is a growing example of cases with an impact on the health system, with PHC being the gateway to the care path and with an important role in early screening for better diagnosis and management, with CH as a technology that facilitates this process.
The increase in diagnosed cases of ASD in Brazil is accompanied by the epidemiological transition, raising numerous questions, ranging from the screening method to the quality of care offered by health professionals. A recent study focused on the care of these children in PHC showed an increase in incidence, especially in socioeconomically more vulnerable communities, in addition, concerns related to screening processes, diagnosis, professional qualification and the need for improvements that enable adequate early intervention were highlighted. (6)
The use of health technologies increasingly helps in acquiring knowledge and updating knowledge. In the context of PHC and the relational dimension, technologies should be used with the aim of strengthening the bond between the multidisciplinary team and the user, being presented through different approaches, with emphasis on educational, managerial and assistance technologies. The conception of technology becomes expanded, transcending the generalized idea that summarizes it to technical and operational procedures, as well as its trivialization. In this way, technology is seen as the sum of everyday experiences and research, resulting in a series of scientific knowledge for the production of materials, in order to enable interventions, based on the evaluation and systemic control of the entire process. (7)
Educational, assistance and management technologies unify theoretical and practical actions with research, building a technical-scientific knowledge that is useful in improving personal and professional relationships, enabling subjects to interfere in their reality through problem solving. As pointed out by a study (8), the technologies available to assist PHC professionals, in the context of growth and development, point to an evolution towards providing options for use, even though they lack better dissemination and strengthening.
Based on the above, the need emerges to help health professionals to expand their knowledge and facilitate the process of child surveillance in practice by strengthening adequate monitoring and identifying possible delays in neurodevelopment at an early stage. Thus, the objective of this study was to develop an educational assistance mobile application for ASD screening in Primary Care.
METHODS
This is a methodological research that addresses the process of developing instruments and strategies, contemplating the methods of obtaining and organizing data, guiding the research. (9) The study was developed in João Pessoa-PB, in the years 2021 and 2022 using the Analysis, Design, Development, Implementation and Evaluation (ADDIE) model, which is divided into small interdependent phases, in which the 'conception' of planning is separated from its 'execution' (implementation and evaluation).
Thus, phase 1 included analysis: it consists of delimiting the educational problem and designing an approximate solution, through situational analysis with a survey of needs and information, being consolidated through a scope review that mapped the technologies available on the subject (8) and a literature review about ASD screening in PHC (9) added publications from the Ministry of Health, such as the Child Booklet and the Autistic Spectrum Disorder (ASD) care line in children, the M-CHAT-R tool and other scientific articles (11-13) which served as theoretical support.
Phase 2: Design: comprised the design planning of the situation itself, through mapping and sequencing of contents, structured by the work of professionals from different areas who work in the same direction to produce a homogeneous solution focused on educational objectives. And, finally, phase 3: prototype development: consists of the production and adaptation of resources and didactic materials, parameterization of virtual environments and the preparation of pedagogical, technological and administrative supports. In this phase, the result of the project is the presentation of content, and it started with the definition of the object, the target audience of the content to be addressed and the definition of platforms to be worked on. The requirements were exemplified in the figure (Figure 1) below:
Figure 1 – Elo Application Requirements. João Pessoa- PB, 2022.
|
R1: Requisitos de BACKEND (API: Application Programming Interface) |
Create database;
Implement access control;
Implement a registration service;
Implement presentation area.
R2:UI (Interface) requirements
Create the login screen;
Create the application splash screen;
Create application menu screen and space for contact;
Create an “Introduction” screen about ASD;
Create ASD “Diagnosis” screen;
Create screen on “Assessing development”;
Create “M-CHAT R/F™” screen;
Create screen on “Risk assessment”;
Create screen on “Putting it into practice”;
Create “Final message” screen.
A3: UI API Integration Requirements
Integrate R1 with R2.
Source: MENDONÇA AG, et al., 2023.
The Elo software will be presented in virtual stores using a logo, created by the product designer, from the following graphic design platforms: Figma and Adobe Illustrator. It will be characterized by the use of a blue colored background, this tonality with representativeness in TEA and illustration of the name of the application that alludes to union and integration centered on the person and uses a symbol of autism that is the puzzle in the letter “o” of the word Elo, aiming, through its different colors and shapes, to show the diversity of characteristics that make up the spectrum of ASD signs, and which, when united, integrate the individual through a better quality of life, inclusion and, above all, respect for diversity. Every illustration created was structured considering the users of this application (health professionals) and the target public of the study, which are infants. Thus, when making the illustration, infants, health professionals and parents/caregivers were considered.
To develop the application, all the steps described below were followed:
Planning Stage: in this stage, the availability of market technologies, development methodologies used, the most relevant programming language for development, as well as, the main platforms for analyzing the number of users, access facilities and post-development use.
Requirements analysis: A survey of functional, non-functional and regulatory requirements of the application that the system must contain was carried out. It stands out as a functional requirement, the implementation of text boxes with information about the autism spectrum disorder. As non-functional requirements, ease and speed of use are highlighted as necessary, as well as broad access and understanding of the developed solution.
Coding: After surveying the definitions in the elaboration of the content through a literature review (10), the collected data were presented in a suitable format to later be encoded in computational language and embedded in the software, in a robust and integrated development environment, according to the requirements defined in the planning phase. The object-oriented programming language paradigm was used, with the dynamism, portability, high performance and security of the Java language.
Development: The way in which the application is used and the quality level of use was considered throughout its development, observing its functions, interfaces, who will interact with them and handle the system. The environment in which the application should be used was taken into account, and a series of points were observed throughout the construction of the tool, as recommended in the literature. (14)
The prototype was produced to run on tablets and smartphones Android and IOS, aiming to simulate the operation of the application through navigations between all screens and redirects. 45 screens were designed and the application will be available in application stores with a specific registration ID for the respective platforms Apple Store and Google Play.
In order to promote a better usability of the prototype presented here, the basic principles followed during the development of the software and valued in this study were considered. They are: minimal user effort; more function recognition than user memory requirement; minimal frustration during handling; increase usage from work patterns and habits; observe tolerance for differences between the people who will use the system; observe changes in the possible environments in which the system will be used; presence of communication interfaces for reporting problems; maximum support for these tasks by the system. (15)
The Elo software was developed with the contribution of a product designer through the provision of a contracted service for the artistic elaboration of the work, thus assigning the copyright to the author as an individual, thus being the owner and responsible for the work in the literary and scientific scope.
The study used public domain information (original articles, publications from the Ministry of Health) as a data source, thus dispensing with the appreciation, analysis and opinion by the ethics committee that regulates research involving human beings.
RESULTS
The technological product has as its initial screen the name of the application and the image of its logo (FIGURE 2).
Figure 2 – Elo Application Login Screen. João Pessoa- PB, 2022.

Source: MENDONÇA AG, et al., 2023.
This screen allows user login by entering email address and password, being able to use facebook registration or create a new registration that will direct to another screen. On this screen, you can access a link “About the app” that directs you to information regarding the objective and purpose of this application.
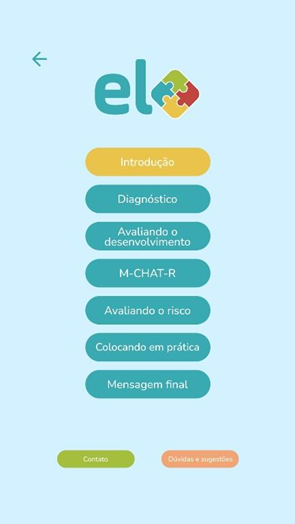
The menu screen (FIGURE 3) presents an expansive menu with multiple choice buttons that direct to topics such as: Introduction, Diagnosis, Assessing development, M-CHAT-R, Assessing risk, Putting into practice and Final message.
Figure 3 – Elo Application Menu Screen. João Pessoa-PB, 2022.
Source: MENDONÇA AG, et al., 2023.
The screen (FIGURE 4) suggests the use of the Child Booklet, available in “boy” and “girl” versions, featuring buttons with different colors (blue and pink respectively) to access them.
Figure 4 – Diagnostic Screen and CB link. João Pessoa- PB, 2022.

Source: MENDONÇA AG, et al., 2023
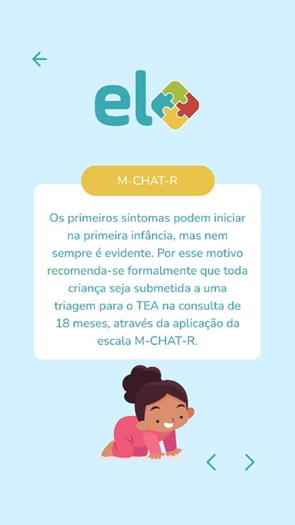
The screen (FIGURE 5) shows the definition of the M-CHAT-R scale and its recommendation for application in the 18-month consultation, as a screening tool for ASD available in the child's Booklet.
Figure 5 – M-CHART-R definition screen. João Pessoa- PB, 2022.
Source: MENDONÇA AG, et al., 2023
Specifically on the “registration” screen, information appears with which will compose the application user registration, such as: email address, password, password confirmation, city of origin, state and “I am”; This information is mandatory. The item “I am” comprises information about the user if it is a doctor, nurse, parents, healthcare student, caregiver, or other healthcare professional. It also describes on this screen, the option as mandatory filling on reading and agreement with the Terms and conditions and privacy policies, in addition to the acceptance of terms and conditions and privacy policies in accordance with the provisions of Law No. 13.709/2018 and Civil Framework of the Internet.
The "introduction" button describes the definition and prevalence of Autism Spectrum Disorder (ASD), etiology, risk factors and the care line published by the Ministry of Health. (11) The "diagnosis" option shows warning signs, the environment for ASD diagnosis, a link to the Child Booklet, complementary exams and comorbidities. In the option "assessing child development", it emphasizes the importance of monitoring developmental milestones in hearing, vision and aspects of the motor system. "Assessing the risk" mentions the legislation that makes the application of a screening tool mandatory in children for developmental alterations, the statement appears that the scale is not diagnostic, presents the correlation of the response in the scale and its score, describes the possibility of false-negative results and the course of action to be taken in these cases, and which cases are considered positive and the course of action to be taken. The "putting it into practice" button at this point allows the application of the M-CHAT-R/F scale that is available in the child's Booklet, which can be viewed widely by scrolling the screen and generating, after completing items 1 to 20, a final sum displayed, the final score and the conduct determined in a box available at the end of the screen. Finally, as a "final message" in which the importance of using a tool as a screening tool for early diagnosis and intervention is emphasized. It also suggests the use of the Child's Booklet as an important tool for approaching child health.
In this way, the Ello application comprises a total of 45 access screens that allow accessibility and dissemination of knowledge, strengthening the health professional-user-family bond in health care, proposing to be inserted in the context of early screening of children with ASD.
DISCUSSION
The development of technological tools enables accessibility, integration and greater care management. With the advancement of the inclusion of technologies in the health scenario, there was less distance in the user-health professional interface, positively impacting the assistance provided, which became safer and more assertive. (16) Among technologies, applications are of great importance, being developed and used in teaching health professionals and patient self-management. (17,18)
Through a scope review (8) which object of study were instruments for monitoring the growth and development of infants, it was identified that the highest number of results from tools with scientific evidence are applications, being primarily intended for users of the health system, and that when they have a care purpose, they have difficulties in integrating systems that operate at the interface between users and health professionals.
Studies reinforce that applications with an educational focus should be encouraged because they contribute to learning that supports care practice, however this contribution must be critically analyzed because it does not guarantee the best learning on its own, but rather an instrument that favors autonomy and cooperation in the knowledge process. (16) Educational applications favor access to knowledge to health professionals from remote areas and promote improvement in the quality of service provision for the assisted population. (16) However, funding, operational sustainability and technology availability are challenges highlighted. (18) The use of an application in the health area can help parents to incorporate good health habits, thus modifying behavior. (19)
In general, mobile care technologies enable, in addition to qualified therapeutic guidelines, reliable diagnoses, as well as the acquisition of experience by undergraduates and empowerment of patients by encouraging self-care practices and strengthening the care bond with users and family members. (20) In healthcare, more than 165,000 mobile apps have been made available through iTunes and Android app stores since 2015 and 34% of mobile users had at least one health-related app on their device. (20) Another data that confirms the accessibility of these devices, published in 2018 by the National Household Sample Survey (PNAD - Pesquisa Nacional por Amostras de Domicilio), is that the cell phone is the type of equipment most used to access the internet at home and is present in more than 99.2% of homes in the country. (21)
According to the 2019 Global Mobile Consumer Survey, in most developed countries, around 90% of adults own a smartphone, with around 95% of these smartphones being used daily. (21) This example of Information and Communication Technology (ICT) has been standing out for enabling communication and numerous functionalities, offering the user an efficient operating system and easy access to the internet. (20)
On the other hand, as an important example of a robust and underused tool, there is the Child booklet, which shows low awareness of health professionals for filling it out, being seen as a bureaucracy of the service, showing absence of the instrument in the health services, weaknesses in the communication process and devaluation of the use of the booklet by the family members. (23,24) In the context of analysis of monitoring and child surveillance, the non-involvement of family members in this practice of CB use, it is also referred to by family members as a failure to communicate with health professionals with prejudice to the child's development due to the non-inclusion of caregivers in this action, exposing weaknesses and increasing the vulnerability of the child's universe. (25,26)
The developmental surveillance process is related from promotion to the detection of problems in normal development in primary health care for children. It is a continuous process and is influenced by health professionals, parents, caregivers, teachers and others. In the APS, the monitoring of child development is consolidated and it is able to identify early changes that may impact the future. This occurs mainly through educational actions and the integral follow-up of the children. (27)
In this context, reinforced by public policies centered on the axis of growth and development and people with disabilities, in the law for the protection of the rights of people with ASD nº 12.764/2012 (28), and in the line of care for children with ASD published by the Ministry of Health, the health technology of the Caderneta da Criança brings in its new digital version a screening tool for ASD, which consists of a questionnaire intended for parents and caregivers and facilitated by health professionals, the M-CHAT-R/F (Modified Checklist for Autism in Children). This tool is validated, free, easily accessible and widely used, capable of identifying warning signs in the child's neurodevelopment through scores.
This scale corroborates the early diagnosis and screening of signs of atypical development that direct towards initial interventions and better quality of life for children. For greater applicability of the scale, it was translated into Portuguese and the M-CHAT questionnaire was validated, taking into account cultural and linguistic differences. (29) The translation of this questionnaire and its adaptation into Portuguese was of paramount importance, as there were few possibilities for health technologies that would corroborate the diagnosis of ASD in Brazil. However, studies are still needed to understand all the cultural diversity of our country, which is so extensive territorially and complex from a neurolinguistic perspective.
In recent scope review (30) which analyzed the availability of diagnostic tools for early screening of ASD in PHC, as a result of which several studies were found, which effectively accelerate the process of diagnosis and initiation of personalized therapy, however, they have significant limitations as some are available only for research purposes, while others lack scientific evidence to prove their effectiveness.
Other studies converge on the understanding that the warning signs in neurodevelopment should be perceived in the first years of life, until around 3 years of age, it is important that health professionals in the child follow-up are aware of developmental milestones and behavioral changes for the diagnosis of ASD at an earlier age, and consequently an early referral for behavioral interventions, thus contributing to the prevention of loss of normal functionality and better results in relation to the maintenance of normal brain neuroplasticity. (10)
The M-CHAT-R/F showed greater specificity and positive predictive value when compared to other screening instruments for ASD at 18 months of age. (31) Similarly, studies (32) analyzed the relevance of the M-CHAT-R as it provides important information for the diagnosis of ASD and confirmed that this scale is the most accurate instrument that allows for early screening and monitoring of the symptoms of the disorder. Children with a family history of ASD are three times more likely to be at risk of developing a neurodevelopmental disorder. (33)
A Chilean study that validated the M-CHAT-R/F as a screening technology for early detection of ASD obtained an Alpha reliability of 0.889, Discriminant sensitivity and specificity of 100% and 98%, and concurrent ones were 100% and 87.5% respectively. (34) In view of the literature analysis, this screening scale and its variations have high sensitivity and reliability to corroborate the diagnosis of ASD. Thus, the implementation of this scale in the Children's booklet facilitated access to this instrument by professionals, also facilitating the initial approach and continuous follow-up of these patients by health professionals.
In the meantime, there has been the important development of the Elo software as a mobile application of an educational and assistance nature, filling gaps and ratifying the robust child surveillance instrument of the Child's Booklet, proving to be an innovative tool for disseminating knowledge about risk screening for ASD and the use of a scale that facilitates this screening and thus enables a greater positive impact on child health.
By reducing vulnerabilities and minimizing fragility, the Elo mobile application favors that the educational and care practice is centered on the prevention and early detection of changes in child growth and development, also favoring the link between parents and/or caregivers with PHC health professionals. Screening evaluations with parents and caregivers favor that the collected information is more accurate and allows for more assertive behaviors. (35) This software also meets the demand for the inclusion of new technologies for the SUS in an agile, intuitive and positive way, providing access to knowledge and better quality of care.
CONCLUSION
The development of the Elo educational assistance mobile application for ASD screening in Primary Care is an important educational and assistance tool for child surveillance to train health professionals in monitoring early childhood, in addition to presenting an innovative character, since there is no similar tool that allows subsidizing the use of the child's booklet and the monitoring of child growth and development, favoring the early identification of warning signs for ASD in an accessible and intuitive way.
The relevance of the study lies in its contribution to the production of new health technologies, such as mobile applications, to strengthen CB itself and the specific line of care for ASD in all of the care network, positively impacting the quality of life of children with ASD. The next step is to carry out a validation study of this mobile technology for subsequent pilot testing and implementation with robust scientific evidence and acquired knowledge.
REFERENCES
1.Caldas GRF, et al. Puericultura na atenção primária a saúde: problemas evidenciados pelos enfermeiros. Saúde Coletiva (Barueri), 2021; 11(61):4784-4797. Disponível em: https:/doi.org/10.36489/saudecoletiva.2021v11i61p4784-4797
2.Rosolem LH, et al. Caderneta de saúde da criança: coordenação do cuidado e acesso à saúde. Cogitare Enfermagem, 2019; 24: e61496. Disponível em: http://dx.doi.org/10.5380/ce.v24i0.61496
3.Caminha MFC,et al. Vigilância do desenvolvimento infantil: análise da situação brasileira. Revista Paulista de Pediatria, 2017; 35 (1):102-109. Disponível em: https://doi.org/10.1590/1984-0462/;2017;35;1;00009
4.Pedraza DF, Santos IS. Avaliação da vigilância do crescimento nas consultas de puericultura na Estratégia Saúde da família em dois municípios da Paraíba, Brasil. Epidemiologia dos Serviços de Saúde, 2017; 26(4):847- 855. Disponível em: https://doi.org/10.5123/S1679-49742017000400015
6.Salgado NDM, Pantoja JC, Viana, RPF, Pereira RGV. Transtorno do Espectro Autista em Crianças: Uma Revisão Sistemática sobre o Aumento da Incidência e Diagnóstico. Research, Society and Development,2022; 11(13): e512111335748.Disponívelem: http://dx.doi.org/10.33448/rsd-v11i13.35748
7.Nietsche EA, Backes VMS, Colomé CLM, Ceratti RN, Ferraz F. Tecnologias educacionais, assistenciais e gerenciais: uma reflexão a partir da concepção dos docentes de enfermagem. Rev Latino-am Enfermagem 2005 maio- junho; 13(3):344-53. Disponível em: https://www.redalyc.org/articulo.oa?id=281421844009
20.Silva AMA, Mascarenhas VHA, Araújo SNM, Machado RS, Santos AMR, Andrade EMLR. Mobile technologies in the Nursing area. Rev Bras Enferm [Internet]. 2018;71(5):2570-8. Disponível em: http://dx.doi.org/10.1590/0034-7167-2017-051
22.Deloitte Touche TohmatsuLimited. 2016. Mobile ConsumerSurvey: hábitos dos usuários e tendências para o mercado de telecomunicações. 2016. Disponível em: https://www2.deloitte.com/br/pt/pages/technology-mediaand-telecommunications/articles/mobile-survey.html. Acesso 11 jun. 2022.
23.Almeida AC, Mendes LC, Sad IR, Ramos EG, Fonseca VM, Peixoto MVM. Uso de instrumento de acompanhamento do crescimento e desenvolvimento da criança no Brasil: Revisão sistemática de literatura. Revista Paulista Pediatria, 2016; 34: 122-131. Disponível em: https://www.scielo.br/j/rpp/a/kT3hnH3L8xRfKDVVBQ6dnjC/?format=pdf&lang=pt
24.Silva FB, gaíva MAM. Dificuldades enfrentadas pelos profissionais na utilização da caderneta de saúde da criança. Revista Brasileira de Pesquisa em Saúde,2017; 18 (2):96–103. Disponível em: https://periodicos.ufes.br/rbps/article/view/15089
25.Bezerra ICS, et al. Análise das ações de vigilância do desenvolvimento infantil segundo cuidadores de crianças. Revista Brasileira de Ciências da Saúde, 2020; 24 (3):e50218. Disponível em: https://doi.org/10.22478/ufpb.2317-6032.2020v24n3.50218
28.Brasil.Lei nº 12.764 de 27 de dezembro de 2012. Política Nacional de Proteção dos Direitos da Pessoa com Transtornos do Espectro Autista. Presidência da República, Casa Civil.
33.Ben-Sasson A, Robins D, Yom-Tov E.Risk Assessment for Parents Who Suspect Their Child Has Autism Spectrum Disorder: Machine Learning Approach. JournalofMedical Internet Research, 2018; 20 (4):e134.Disponível em: https://doi.org/10.2196/jmir.9496
35. Montenegro KS, Figueiredo MAB, Castro LSF, Kietzer KS. Aplicativo sobre a detecção precoce do autismo: uma ferramenta educacional para o ensino em saúde. Revista Eletrônica Acervo Saúde, 2019;11(6): e347.https://doi.org/10.25248/reas