ISSN Eletrônico - 2675-0244
ISSN Impresso - 1806-3365
RESUMO
Objetivo: elaborar fluxograma como ferramenta tecnológica de reorganização da atenção à saúde do homem. Método: pesquisa metodológica que envolve a investigação dos métodos de obtenção e organização de dados e o desenvolvimento/construção de fluxogramas referentes a atenção à Saúde do Homem nas unidades de saúde da família e demais órgãos de atendimento à saúde da população masculina do município de João Pessoa - PB. O estudo foi desenvolvido em quatro etapas: revisão bibliográfica e coleta de dados; diagnóstico situacional; construção dos fluxogramas e submissão dos fluxogramas ao processo de edição e diagramação. Resultado: uma análise de cada fluxograma e sua aplicação, sugere melhorias do serviço na atenção à saúde do homem. Conclusão: ressalta-se a importância desta tecnologia para os profissionais e usuários do sistema de saúde nas unidades objeto do estudo.
DESCRITORES: Atenção Primária à Saúde; Saúde do Homem; Políticas Públicas; Gestão em Saúde.
ABSTRACT
Objective: to elaborate a flowchart as a technological tool for the reorganization of men's health care. Method: methodological research that involves the investigation of the methods of obtaining and organizing data and the development/construction of flowcharts referring to men's health care in family health units and other health care bodies for the male population in the city of João Pessoa - PB. The study was developed in four stages: bibliographic review and data collection; situational diagnosis; construction of flowcharts and submission of flowcharts to the editing and layout process. Result: an analysis of each flowchart and its application suggests service improvements in men's health care. Conclusion: the importance of this technology for professionals and users of the health system in the units under study is highlighted.
DESCRIPTORS: Primary Health Care; Men's Health; Public policy; Health Management.
RESUMEN
Objetivo: elaborar un flujograma como herramienta tecnológica para la reorganización de la atención a la salud del hombre. Método: investigación metodológica que involucra la investigación de los métodos de obtención y organización de datos y la elaboración/construcción de flujogramas referentes a la atención a la salud masculina en las unidades de salud familiar y otras instancias de atención a la población masculina en la ciudad de João Pessoa - PB. El estudio se desarrolló en cuatro etapas: revisión bibliográfica y recolección de datos; diagnóstico situacional; construcción de flujogramas y sometimiento de los flujogramas al proceso de edición y diagramación. Resultado: el análisis de cada flujograma y su aplicación sugiere mejoras en los servicios de atención a la salud masculina. Conclusión: se destaca la importancia de esta tecnología para los profesionales y usuarios del sistema de salud en las unidades estudiadas.
DESCRIPTORES: Atención Primaria de Salud; Salud Masculina; Políticas Públicas; Gestión Sanitaria.
INTRODUCTION
Attention to men's health was not among the priorities of government and national health policies for many years compared to public policies aimed at women's health, which have a growing approach in studies, projects and actions. This reality generates serious problems for comprehensive male health care, especially in Primary Health Care (PHC) services, gateway to the health system, which still focus their actions predominantly on the female, child and elderly population, causing men to distance themselves from these services. (1)
In the discussions that gave rise to the National Policy for Integral Attention to Men's Health (PNAISH - Política Nacional de Atenção Integral da Saúde do Homem), the state's omission in men's health care was recognized, whose care was for a long time relegated to a secondary role by health care services, whether due to cultural, social, physiological and/or professional factors, noting that the basic care model for the four population groups – children, adolescents, women and the elderly – is not enough to make the country healthier, mainly by leaving out no less than 27% of the population. (2)
Men are more vulnerable to diseases, serious and chronic illnesses, and do not seek primary care services, entering the health system mainly through outpatient and hospital care, of medium and high complexity, which aggravates morbidity and generates higher costs for the health system. A large part of men's non-adherence to comprehensive care measures, according to the Ministry of Health, stems from cultural variables, such as gender stereotypes, rooted for centuries in patriarchal culture, their beliefs and values of what it means to be masculine. (3)
There is, therefore, a perception that the male population lacks specific care in view of their needs, and that the representativeness of this portion in health services should be encouraged by professionals in the various points of care, in particular, in PHC, for the effective change of cultural paradigms. (4) However, for this to happen, it is necessary to reorganize health actions, through an inclusive proposal, in which men and health services are brought together. (5)
Considering the factors already mentioned, which range from the cultural aspect and its influence on the feeling of invulnerability, as well as the need to adapt the distribution of health services according to the demands and needs of the male population, whose high morbidity and mortality implies demographic inequalities and social phenomena, the need to build a flowchart of care was identified in order to guarantee comprehensive and continuous care throughout the care network, with the health services existing in the city of João Pessoa-PB being chosen as the focus of the study.
Therefore, this study is justified by the gap in the production of scientific knowledge regarding men's health care at different points of care. In this direction, this study focuses on the following questions: are the health services in the city of João Pessoa organized for men's health care? To what extent can the flowchart contribute to the organization or reorganization of the men's health care network? Thus, the objective of the study is to elaborate a flowchart of care for the male population of the city of João Pessoa-PB as a technological tool for the reorganization of men's health care.
METHOD
It is a methodological research, which involves the investigation of the methods of obtaining and organizing data and conducting rigorous research. This type of study deals with the development, validation and evaluation of research tools and methods. (6,7)
It was developed in 2018, thus being based on past data, and retrospectively followed until the moment of this study. For this research, only the instrument development stage (flowchart) was considered, revealing the importance of the data and its relevance at the present time.
The municipality of João Pessoa, capital of the State of Paraíba, was the chosen location for the study because it is in the process of implementing the PNAISH and because it has a technical area dedicated to men's health.
The construction of the flowcharts was developed in the health context of João Pessoa, based on the National Register of Health Establishments (Cnes) - DataSUS, which contains the description of the institutions, units and services provided, based on the data presented by the IBGE in 2018, such as population evolution and morbidity and mortality rates and their comparisons by gender (age pyramid) and scientific articles that reference the construction of the flowchart instrument. (8-10) The study was carried out in four stages:
A search was carried out in the Virtual Health Library (VHL) between January and March 2018, using the descriptors: “primary health care”; "men's Health"; and “health management”, which were grouped together. Inclusion criteria: studies and/or documents that addressed the organization of men's health care and that were available in full and free of charge, without time frame. Bibliographical references cited in selected publications were also used, and manuals from the Ministry of Health were included that portrayed men's health and/or addressed the construction of flowcharts or the organization of men's health care in health services.
All health services that are part of the health care network in the city of João Pessoa were identified, among which those that refer to men's health care services were addressed.
The municipality of João Pessoa has a population of 800,323 inhabitants(11), to which, according to the information obtained in the National Register of Health Establishments (Cnes) - DataSUS, coverage of the Family Health Strategy (ESF) is ensured, corresponding to 88.3% of the resident population, distributed in 180 Family Health Teams, which occupy physical spaces in 125 health units.
As components of the primary care network, there are 05 regionalized units (Basic Unit of Mandacaru, Health Unit of Praias, Lourival Gouveia de Moura, Maria Luíza Targino and Health Unit Francisco das Chagas) that act as a reference for the population.
Consultations and procedures are also offered at the basic clinics of the Integral Health Care Centers (CAIS - Centros de Atenção Integral à Saúde) in the neighborhoods of Mangabeira, Jaguaribe and Cristo, with units of the Community Health Agents Program (PACS - Programa de Agentes Comunitários de Saúde) in the neighborhoods of Colibris, Planalto da Boa Esperança, Paratibe, Cidade Verde Colinas do Sul, Jaguaribe and Bessa.
Specialized hospital and outpatient care services are referenced by the Gateways and ordered by Primary Health Care, according to the assessment of the severity of the individual and collective risk, the waiting time and, observing the specificities foreseen for people with special protection, according to current legislation.
The specialized care network comprises the following services: Integral Health Care Centers (CAIS): Jaguaribe, Mangabeira and Cristo; Praias and Mandacaru Health Unit and Specialty Dental Centers (CEO’s - Centros de Especialidades Odontológicas) in the neighborhoods of Torre, Mangabeira and Cristo. There are also the Integral Health Care Centers for the Elderly – CAISI, the Municipal Central Laboratory (LACEN - Laboratório Central Municipal) and the Testing and Counseling Center (CTA - Centro de Testagem e Aconselhamento) for STD-AIDS.
The mental health network is made up of Psychosocial Support Centers (CAPS - Centros de Apoio Psicossocial): CAPS III Gutemberg Botelho, CAPS III Caminhar, CAPS I Cirandar and CAPS AD Davi Capistrano, for the Mental Health Emergency Room (PASM - Pronto Atendimento em Saúde Mental), Child Care Unit, Residential Therapeutic Services – Tambiá and Mandacarú and Office on the Street.
In compliance with the principles and guidelines of the National Workers' Health Network (RENAST - Rede Nacional de Saúde do Trabalhador), there is the Reference Center for Workers' Health - (CEREST - Centro de Referência em Saúde do Trabalhador) Regional, directed towards actions related to workers' health.
Specialized care is also offered in outpatient clinics at municipal hospitals: Complexo Hospitalar Mangabeira Tarcísio Burity; Cândida Vargas Institute, Hospital Municipal Santa Isabel and Hospital Municipal Valentina. João Pessoa's pre-hospital care is structured based on the Emergency Medical Care Service (SAMU - Serviço de Atendimento Médico de Urgência), in compliance with the guidelines of Ordinance 2048/MS, with the aim of providing mobile pre-hospital care. The network also has 03 Emergency Care Units (UPA - Unidades de Pronto Atendimento), located on the beaches (Oceania) and in the neighborhoods of Valentina and Cruz das Armas, which offer 24-hour emergency care.
The SUS hospital network belonging to the Municipality of João Pessoa is distributed in 4 institutions: Santa Isabel Municipal Hospital (medical and surgical clinic), Valentina de Figueiredo Municipal Hospital (pediatric clinic), Cândida Vargas Institute (gynecology and obstetrics, neonatal clinic) and Complexo Hospitalar Municipal Governador Tarcísio de Miranda Burity (elective trauma and orthopedics and emergencies).
Data were collected to prepare the organization chart of the institution, with the indication of the establishments that provide services in the area of primary attention to men's health, on a complementary (non-exclusive) or subsidiary basis, with the exposition of its competences and location, in order to describe the paths taken by the user from the PHC to the other points of care. The collection of data on the components of the municipal health network and the indication of the flows found was elaborated based on data from the CNES and scientific articles, from January to March 2018. (8,9-12)
It is important to highlight that during this study, the elaboration of flowcharts in the area of men's health at the municipal level was not found in the literature or on the official websites of the health department itself, as explained in the justification and exposition of the objectives of this work, previous actions are related to care for other population segments, which reinforces the importance of this study for the male population served in this municipality.
It is also reinforced that, although the study was carried out in 2018, the purpose of this work was not to portray only one branch of health care, like other flowcharts presented in the literature and in the analyzes of public health institutions, but a whole structure focused on men's health in accordance with the PNAISH guidelines, understanding the points of care, the multiplicity of existing situations and injuries and the distribution of care branches according to the age group of the population, hence simplification was the path used, precisely because the flowchart must be self-explanatory, which would be unfeasible if it contemplated all possible situations.
For these and other limitations, but also for understanding that the definition of some processes can serve as a pretext for a more complex approach, as well as to spread the interest in the continuity or even expansion of this theme among the teaching and student bodies, or even the management itself , this work chose to carry out the instruments paying attention to the following aspects - Flowchart 1: general flowchart of men's care in the Family Health Units; Flowchart 2: flowchart of access and reception to the man in the Family Health Units; Flowchart 3: flowchart of the prostate cancer prevention test; Flowchart 4: male external genital examination flowchart; and Flowchart 5: flowchart of the family planning consultation (prenatal) with the participation of the man in the Family Health Units.
Therefore, given the multiplicity of paths, and in order not to make the analysis so complex as to confuse more than clarify, the description was chosen in a broad and general view, which can, obviously, after a future process of validation and improvement , reach other levels of detail by scrutinizing the flows and processes in the direction that knowledge and curiosity point.
The health context of João Pessoa was associated with data from the literature and with the thematic axes of the PNAISH, culminating in the construction of flowcharts.
For the construction of the flowcharts, four of the five thematic axes of the PNAISH were approached, related to Access and Reception; Prevalent diseases in the male population; sexual and reproductive health of men; fatherhood and care.
It consisted of submitting the flowcharts to the editing and layout process, following criteria related to content, structure/organization, language, layout and design, cultural sensitivity and adequacy to the local health context.
The layout of the figures follows the pattern adopted in the literature, with the arrow being the symbol that indicates the connection between other symbols, as well as the direction of the flow of the processes included therein. The termination (rectangle with circular sides) indicates the start or end of a flow in the diagram. The rectangle indicates an involved process and its activities. The diamond indicates a decision-making process, from which different directions are adopted, indicated by arrows. The connector indicates an inspection is to be performed.
All flowcharts start with the termination symbol, which indicates the input of the analyzed process, in the case of the present study, the male population and the age groups distributed in it. Each institution, unit or component of the health care network was indicated as being a process, considering that activities are carried out in them involving users and professionals involved in each stage of care in health care (primary, secondary and tertiary), in a way that they do not represent static elements, but a set of actions and activities performed for the benefit of the user, which may or may not mean the end of the primary health care process, with arrows being used to point out the preferential flow of the user in the system during the evolution of care from the basic network to the most advanced levels of technical complexity in the network.
Finally, the symbol used in decision-making was only used to indicate the hypotheses in which the process follows different paths from a finding, technical or clinical (as in the flowchart of prevention and treatment of prostate cancer), obviously considering that in health care, in each action, step or process there are a series of decisions to be taken.
RESULT
Knowing the institutions involved, their functions, distribution, location and purposes, by itself, already represented a herculean task, demanding no less effort to indicate the references and procedures carried out in each of them, whose knowledge allowed the interweaving between the care networks in their care points, resulting in the cognitive framework for the preparation of instruments related to the care and reception processes, represented by a summarized organizational chart of the institutions belonging to the Municipality.
The elaboration of the flowcharts involved deepening the technical and political relations of public management initiatives, in order to understand that not only in spreadsheets and statistics are the reasons for the implementation of this or that structuring health equipment in this or that locality. The analysis of the flows and procedures exposed in the flowcharts sought, in all its phases, to simplify the routines and the visual lightness of the graphics, so that they are the object of constant consultation and application, even by those who do not have an advanced level of knowledge, behold, in a comprehensive way, they are intended perhaps for users of the health care service for the male population.
Once the flowcharts were made, the challenge had just begun. It is understood that the completion of the work will only be achieved after the validation process of the instruments by professionals in the area and experts with recognized ability to optimize management processes, at the same time that it will serve, in the future, as a basis for the necessary planning for the expansion of the municipal public health network.
In this context, and based on the distribution of services in the Health Care Network of João Pessoa/PB, the organization chart of the municipality was prepared, indicating the health establishments that provide services in the area of primary care for men's health, exposing their competences, areas of activity and location, in order to describe the paths taken by the user from the PHC to the other points of care (Figure 1).
Figure 1 – Organization chart of men's health care in the city of João Pessoa-PB, 2018.

Source: Research data, 2018.
The organization chart of men's health care in the city of João Pessoa/PB, together with the definition that the male population (children - under 12 years old; adolescents - between 12 and 18 years old; adults - between 18 and 59 years old; and elderly - over 60 years old) is the input of the care network, they are the elements used in the elaboration of a flowchart with the idealization of the flow of human health care.
In order to reinforce the importance of Primary Health Care (PHC), a general flowchart of men's care in the Family Health Units was created (Figure 2).
Figure 2 – General flowchart of men's care in Family Health Units. João Pessoa, 2018.
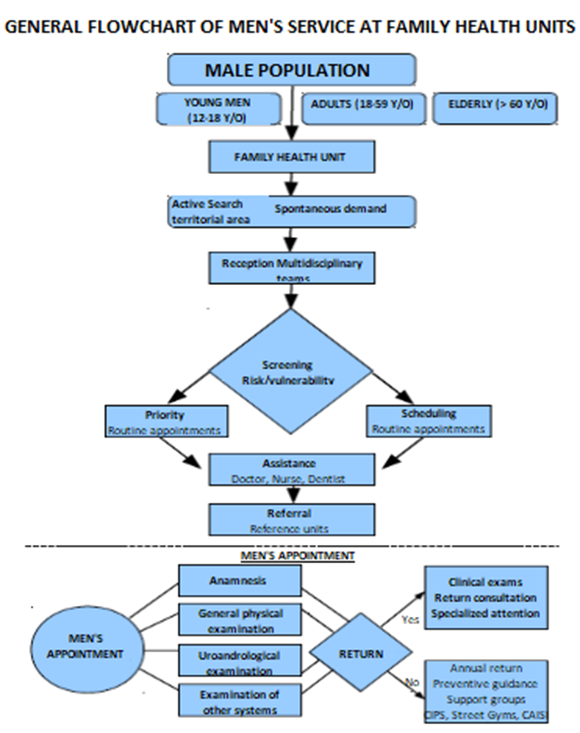
Source: Research data, 2018.
This flowchart considered the age group from 0 to 60 years old in the male population, starting from care with multidisciplinary care to specific care with referral, when necessary for the various specialties.
At the same time, to reinforce the accuracy of quality care for male spontaneous demand in PHC services, the flowchart of access and reception for men in the Family Health Units is exposed (Figure 3).
Figure 3 – Flowchart of access and reception to men in Family Health Units. João Pessoa, 2018.

Source: Research data, 2018.
The flowchart of access and reception for men in the Family Health Units represents a possible strategy for organizing the access and reception of the male population to PHC services, and can be adapted, enriched and adjusted, according to the specificity and characteristics of each territory .
Figure 4 shows the flowchart of the prostate cancer prevention test. João Pessoa, 2018, demonstrates the flows and processes involved in the prostate cancer prevention exam.
Figure 4 – Prostate cancer screening test flowchart. João Pessoa, 2018.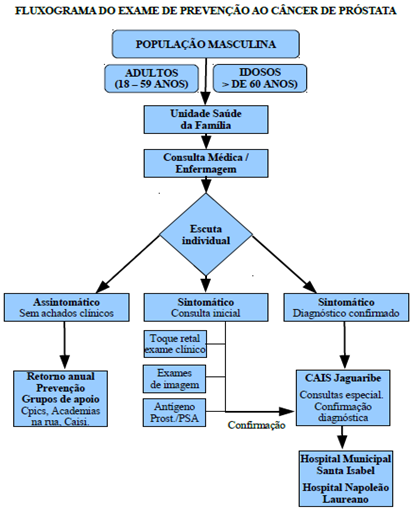
Source: Research data, 2018.
The establishment of a service flow that guarantees the carrying out of screening tests for both prevention, as for the early detection of prostate cancer, it is fundamental for controlling the disease and reducing the high costs resulting from the treatment of this pathology in advanced stages or in metastasis. 13,14
The flowchart of the male external genital examination (Figure 5) addresses an important component of male health care, given the sociocultural characteristics and technical and ethical aspects involved. Given the difficulties encountered in performing the examination of the male external genitalia, this is a unique component for the health team.
Figure 5 – Flowchart of male external genital examination. João Pessoa, 2018.

Source: Research data, 2018.
The flowchart of the family planning consultation (Figure 6), which includes prenatal care with the participation of men in family health units, aims to disseminate knowledge and encourage this policy, as recommended by the PNAISH.
Figure 6 – Flowchart of the family planning consultation (prenatal) with the participation of the man in the Family Health Units. João Pessoa,2018.

Source: Research data, 2018.
DISCUSSION
For men, strength, invulnerability, virility, work and being the head of the family have become, throughout history, one of the factors responsible for the devaluation of self-care, especially when it comes to issues related to the genitals. (15,16)
This observation becomes even more relevant, since different factors push them away or prevent them from seeking health services, especially in primary care, such as: the feminization of the aesthetics of health units, favoring the non-belonging of man to the environment, educational and awareness campaigns that do not address male singularities, the unpreparedness of health professionals to deal with sexual diversity, going beyond the biomedical dimension and often adopting attitudes and values of a personal and moral nature and the lack of policies that assist men when they are companions of users in health units. (17)
We understand, therefore, that the organization of services directly influences the inclusion of men in health services. For this reason, it is essential to raise awareness among professionals so that they promote quality care, through qualified listening, in order to better understand this population regarding their perception of their health. (18)
That said, meeting spontaneous demand in primary care services must be based on the principle of equity, enshrined in the Unified Health System (SUS) through the premise that it is necessary to treat the unequal differently or each one according to their need, avoiding unfair differentiations and the failure to observe different needs. Therefore, teamwork is fundamental, starting from reception, in which everyone can identify situations that present a greater risk or that generate intense suffering. (19,20)
Continuing with the approach to the men's health care network, we entered the analysis regarding the diseases prevalent in the male population, which also represents a thematic axis of the PNAISH, among which we highlight prostate cancer, whose social relevance to justify this choice can be expressed by the high rates of its incidence. This type of cancer is already twice as frequent as breast cancer. 21 Hence the importance of prevention and early detection, to ensure quality of life and adequate treatment in maintaining health and disease control.
With regard to the genitals, although men and health professionals are not in the habit of examining the external genitalia, this self-care is necessary for the prevention and early detection of penile and testicular cancer, which has increased considerably in recent years. 22
In Brazil, the regions with the highest incidence of these pathologies are the North and Northeast, affecting mainly elderly men, in the case of penile cancer, and men between 15 and 50 years of age, in the case of testicular cancer, regardless of their ethnic origin, being directly linked to low social status and poor hygiene habits. 23
Making investments in the training of health teams is essential for the guidance, care and recovery of this user 23,24, based on the construction of a flowchart as a service improvement technology, it represents an adequate tool for this purpose.
Finally, focusing on another thematic axis addressed by the PNAISH, which deals with attention to men in prenatal care, It should be noted that since the enactment of Law No. 11,108, of April 7, 2005, pregnant women were guaranteed the right to the presence of a companion during labor, delivery and immediate postpartum, within the scope of the Unified Health System - SUS, which is why it was also important to analyze, through a flowchart, the family planning consultation (prenatal) with the participation of the man in the Family Health Units, recognizing the importance of this involvement, including its socio-affective repercussions on other cycles of the child's and family's life, and even more so the lack of other studies on the specific topic.
In this direction, aiming to increasingly promote the conscious and active involvement of adolescent, young, adult and elderly men in all actions aimed at reproductive planning, and as a consequence, improve and expand this group's access and reception to health services, the Ministry of Health has invested in innovative tools, such as male prenatal care. 24 Aiming to increase the man's sense of belonging to the family and strengthen the man-woman and father-child bond, even having consequences in the reduction of domestic, physical and psychological violence. 25
That is why the importance of establishing a service flow that also involves family planning with active male participation and not just as a mere auxiliary, or financial support, contributing to the reduction of gender differences, through the involvement of men in sexual and reproductive health and sharing responsibilities with women.
CONCLUSION
Our main perspective during this study was in the sense that the elaborated instruments serve for an effective reorganization of men's health care. The analysis of the flows and procedures exposed in the flowcharts sought, in all its phases, to simplify the routines and the visual lightness of the graphics, so that they are the object of constant consultation and application, even by those who do not have an advanced level of knowledge, as they are comprehensively intended for users of the health care service for the male population.
Having achieved the objectives proposed here, it is expected to evolve in this work, with the validation of the appearance, content and clinic, accepting the recommendations and making the necessary adjustments to an effective contribution of the flowchart as a technological tool for the reorganization of men's health care.
REFERENCES
de câncer. Câncer de próstata. [Internet] 2013 [2023 fev 28]. Disponível em:http://www2.inca.gov.br/wps/wcm/connect/tiposdecancer/site/home/prostata.